THE TRUTH ABOUT LASIK
LASIK does not prevent or treat eye disease. LASIK is a surgical procedure performed on healthy eyes for cosmetic reasons only – to get rid of distance glasses. Eyes are essential, so the rate of serious complications from LASIK should be zero. In fact, the complications are multiple, disastrous, permanent, and untreatable. They include blindness, life-long pain, disability, and suicide.
Eye doctors are supposed to make sick eyes healthy. LASIK surgeons take healthy eyes and make them sick. There is nothing wrong with eyes that need glasses. They see well with glasses before the procedure. They ought to see equally well after the procedure, but they do not. Patients are not warned about this. They have no idea they are gambling with their most precious possession – their vision.
One of the suicides caused by LASIK is that of Jessica Starr, a Detroit TV meteorologist. Jessica had everything â- beauty, health, a job she loved, a devoted husband, and two small children – but 2018, two weeks before Christmas and a month after she complained on Facebook about dry eyes, blurred vision, and pain, she killed herself. She had no history of depression.
People like Jessica Starr are gullible. They believe the glowing LASIK ads. They trust the LASIK surgeons. They think doctors will never do them harm. They don’t want to hear bad news. They do not do their homework. Most important, the LASIK surgeons do not warn them about the risks.
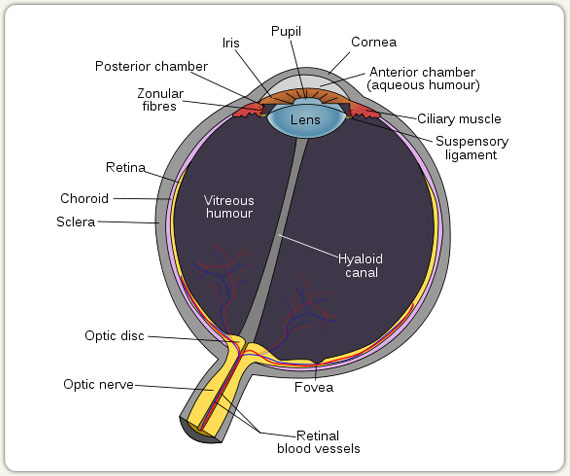
LASIK is a procedure that surgically re-shapes the cornea, the dome shaped, clear structure in front of the eye. Eyes are near-sighted (myopic) because their corneas are steeper than normal. When the cornea is flattened, the near-sightedness goes away.
Radial Keratotomy (RK) was the first surgical procedure devised to flatten the cornea to eliminate near-sightedness. It was invented in 1974 by a Russian, Svyatoslav Fyodorov, flattened the cornea by cutting deep incisions in the periphery. The side effects included unpredictable healing, scarring, vision instability, infection, cataract formation, and irregular astigmatism, so RK was eventually abandoned.
In 1983, a colleague of mine at the Harkness Eye Institute, Dr. Steve Trokel, invented a more sophisticated procedure to flatten the cornea, by using the excimer laser. This laser could re-shape the cornea with mind-blowing precision because it gives off ultrashort (1 to 8 nanoseconds) bursts of ultraviolet light. (A nanosecond is a billionth of a second.) It is a cold laser, so it does not burn tissue. Steve called his procedure LASIK – the acronym for Laser-Assisted in SItu Keratomileusis. (Kerato means “cornea”, and mileusis means “to reshape, in ancient Greek.)
I was one of the first people in the world to hear about LASIK. Steve dashed into my examining room at the Eye clinic in the early 1980s and shoved his now-famous electron microscope photo into my hands. This photo was literally hot off the press – it was still warm. It showed a cornea with an exact rectangle sliced into it by an excimer laser. I was impressed. I toyed with the idea of having this procedure myself, to eliminate my near-sightedness.
When Steve left to show his photo to the eye surgeon next door, I had second thoughts. Steve’s procedure would inevitably cause thinning and scarring of the cornea, which would damage vision. It would inevitable cut corneal nerves, so the patients would develop severe eye pain. I was convinced it would never catch on.
Wrong. I had underestimated how much people want to get rid of glasses. I also did not predict LASIK surgeons would suppress the truth about LASIK, and my fellow ophthalmologists would refuse to speak up.
I have used the Argon, YAG and Selective laser for forty years to save or restore the sight of thousands of eyes. I never have, and never will, use the excimer laser to re-shape the cornea.
The FDA approved LASIK in 1998, and an epidemic of eye pain and damaged vision began to spread around the world. I started to see LASIK patients in my office who were happy. I also saw LASIK patients whose eyes, and lives, were ruined. Damaged LASIK patients have cried in my office, telling me they trusted their LASIK surgeon, but he betrayed them and never warned them this could happen to them.
The head of the FDA committee that approved LASIK was Dr. Morris Waxler, who was the scientist in charge of clinical research trials. After Morris retired from the FDA, he began to see more and more LASIK patients who had serious complications. He realized something was wrong.
Morris took a second look at the original data the LASIK surgeons submitted to the FDA from the clinical trials. Then he reviewed all the papers on LASIK complications in the scientific literature. (He was able to look at medical research papers not readily available to the public.)
Morris realized the FDA-required clinical trials had only looked at how well patients could read the eye chart. They failed to pick up serious long-term side effects – including night vision problems and chronic dry eye – because the number of patients was small, and the follow-up was short-term.
The LASIK surgeons assured Morris these problems were “temporary side effect”. Morris realized they were permanent and devastating. He had been, in his words, “hoodwinked”.
The original data submitted by the LASIK surgeons showed twelve months after the procedure 60% of patients had fluctuating vision in dim light, 50% had gritty eyes, 40% had sensitivity to light, 20% had fluctuating vision in both dim and bright light, and 15-20% had problems driving at night because of glare and halos.
Morris knew I was one of the few ophthalmologists willing to warn the public about the dangers of LASIK.
I told Dan Dorfman, the infamous CNBC “stock picker”, in 1994 that LASIK is “experimental and unpredictable” with “worrisome complications”, including “over and under correction, fluctuating vision, poor vision at night, and pain”. Bloomberg reported my comments, and the stock price of the excimer laser companies immediately plunged tens of millions of dollars.
I described LASIK complications on CBS in May 2008. The LASIK surgeons retaliated by claiming I was “naive” and did not know what I was talking about.
Morris invited me to come with him to Washington, D. C. on September 22nd, 2010, to testify before the FDA about the dangers of LASIK.
As Morris and I rode up the gleaming escalator of the just-opened main building of the brand-new FDA complex in Silver Springs, Maryland, I thought it would be a slam dunk to convince the FDA to ban LASIK. Dazzling minds must work in this dazzling palace. LASIK was a serious public health problem. Once the regulators knew the facts, they would surely ban LASIK.
Morris told the FDA about the misleading statistics that tricked him into recommending LASIK, and why he now believed it should be banned. I explained how the cornea behaves when it is wounded, and why the side effects are unavoidable. I also described patients whose lives were permanently destroyed by this procedure. ABC ran a special about Morris’s testimony that evening.
Three months after our testimony, January 6, 2011, Morris filed a citizen’s petition with the FDA. It is thirty-two pages long. It includes ten figures, six tables, and one hundred and one references from peer-reviewed scientific literature. Every statement is based on scientific research. Now that is good science. It is readily available online – simply Google Morris Waxler FDA LASIK.
His petition states “LASIK eyes never completely heal, are permanently weakened, vulnerable to trauma and inflammation, develop neuropathic dry eyes, have pathology that progresses annually, are vulnerable to blinding corneal bulging, have compromised night vision, have unstable vision corrections that regress, and require eye care that otherwise would not be needed.”
Morris concluded: “LASIK risks and long-term consequences outweigh the benefit of reduced dependence on corrective lenses”. He urged the FDA to withdraw approval for LASIK, issue a Public Health Advisory and recall all LASIK devices.
The FDA response? A drop in the bucket. The FDA website now recommends LASIK patients obtain a copy of their medical record, including the consent form. It also cautions prospective patients their vision at night will be permanently reduced after LASIK, even if they have 20/20 or better vision in bright light. It also warns that visual outcomes of LASIK decline over time.
The FDA did not ban LASIK.
Morris and I did not give up. Eight years later, on September 13, 2018, we went back to the FDA. This time we brought along two LASIK-damaged patients, and a medical doctor, Nancy Burleson, whose son and only child committed suicide after LASIK.
I asked the committee members if they wanted their legacy to be blindness, pain, and death. I gave everybody a copy of a consent form that explains, in language a layman can understand, the risks of LASIK, with the percent chance for each risk. I told them their duty was either to ban LASIK or require that all LASIK surgeons give their patients this consent form at least two weeks before surgery.
Here is the consent form. Unless otherwise specified, all the statements come from the Waxler FDA Petition.
LASIK IS AN ELECTIVE COSMETIC PROCEDURE
- If you have LASIK, you have a 50% chance of developing “dry eye”. This means your eyes will feel as if sand is pasted under your lids, and they will burn as if they have hot pepper sauce in them. There is a 100% chance this pain will be with you for the rest of your life. The “dryness” is actually nerve pain, caused by damaged corneal nerves.
- You have a 60% chance of developing fluctuating vision in dim light, a 50% chance of glare, a 40% chance of sensitivity to light, a 20% chance of fluctuating vision in both bright and dim light, and a 10-20% chance of difficulty driving at night due to halos around lights and ghost images. These problems will never go away. You may have to give up night driving and going to the theatre and movies. If your job requires functioning in dim light, you may become permanently disabled.
- The LASIK flap never heals completely. You have a lifetime risk the flap can dislocate after minor trauma, and infection can creep underneath the flap.
- The cornea is not inert, like a sheet of plastic. It is a living structure that grows and remodels throughout life. 20% of LASIK eyes are not stable. They either go back to being nearsighted, or go in the other direction and become farsighted, or else fluctuate from one to the other. Some eyes continue to fluctuate in vision for as long as twenty-five years.
- LASIK thins and weakens your cornea, which puts it at 1.5% risk of ectasia, or bulging. As the cornea sags outwards, it becomes steep and warped, and your vision becomes progressively more blurred and distorted. The only way to treat ectasia is with hard contact lenses, or a corneal transplant. Ectasia cannot be corrected by glasses or soft contact lenses. Ectasia can develop twenty-five years after apparently successful LASIK.
- LASIK stretches and damages the retina, so your risk of retinal detachment is forty-two times greater after LASIK.
- LASIK patients develop cataracts fifteen years earlier than normal.
- Even if you see better at distance, you will have other problems you did not have before LASIK. For example, people over forty will have to use reading glasses. There is only a 30% chance you will be able to throw away your glasses, according to a 2009 Consumer Reports survey.
- After you have LASIK, there is a 100% chance you will no longer be able to distinguish between subtle shades of grey. (Yamane et al, Investigative Ophthalmology and Visual Science, 2004: “100% of eyes lose contrast sensitivity after LASIK”.)
- Fifty-five percent of patients are unhappy with their vision seven years after LASIK.
The LASIK consent forms do mention complications, but they do not explain them in simple language that the patients can understand, and they do not give percentages.
If this consent form were given to every prospective LASIK patient, very few people would consent.
LASIK surgeons make more money than other eye surgeons because cosmetic surgery is not covered by insurance, so it is not subject to price limits set by insurance companies. Medicare.com says: “LASIK is not considered medically necessary; therefore, it is not covered. - LASIK.com states: “Most insurance companies don’t cover LASIK. It is nearly always considered an elective or cosmetic surgery.”
When I talk to ophthalmologists in private, they readily admit the dangers of LASIK, but they refuse to criticize this multibillion-dollar industry. They know there will be serious push back.
The New York Times published an article on June 12, 2018, which exposed the dangers of LASIK. The article received over one million page views (one hundred thousand is considered impressive). I made this article happen, with the help of a retired NYT editor. I guided the writer, Roni Caryn Rabin, through the laborious process of making sure each statement was backed up by peer-reviewed science. She quoted me in the article. Two days later I appeared on “Good Morning America.”
Today, most people have forgotten about it.
The assault from my colleagues was swift, personal, and lacking in scientific evidence. One ophthalmologist accused me of “fake news” and said I am “no scientist.” Several colleagues pointedly ignored me at a professional meeting. One told me I wasn’t qualified to criticize LASIK because I am a retina specialist. Three filed letters of complaint with the president of the society.
Notably, however, no one disputed the facts: LASIK always causes complications, some mild, some so severe they have led to suicide.
Let’s look at how LASIK is performed, and you will understand why the complication rate is so high.
1) LASIK surgeons begin by flattening the eye with a suction ring, squeezing this delicate structure in a vise. The pressure inside the eye shoots up to over sixty, while normal is between eight and twenty-two. This stretching weakens the retina. The rate of retinal detachment in normal eyes is .006%. After LASIK, the rate shoots up to between 0.25% and 0.36% (see www.eyeworld.org/article.php?sid=4164).
The lens gets squashed also, so LASIK patients will develop cataracts that need surgery fifteen years earlier than people who have not had LASIK.
2) Next, the surgeons slice a flap from the cornea using a knife or femtosecond laser, as if they were cutting a slice off a loaf of bread.
3) Then they use an excimer laser to shave tissue off the center of the cornea. Before LASIK, corneas have a single smooth curve – a perfect dome. After LASIK, this “dome” gets transformed into a “plateau”.
4) Finally, they put the flap back on, and assume it will seal back normally.
It never does.
Schmack et al reported in the Journal of Refractive Surgery in 2005 that the LASIK flap tensile strength is a shocking 2.4% of normal. In the same journal, in 2004, Percy Amoils stated the corneal flap after LASIK provides no more strength than a contact lens. Kramer et al in Cornea, 2005, found faulty healing in every flap they examined under the microscope.
The LASIK flap is attached so weakly that even mild trauma – rubbing the eye, being hit by a wave, contact sports – can dislocate it. When the flap comes off, the eye instantly loses vision. The dislocated flap must be replaced surgically as soon as possible. It is now far more likely to dislocate again.
I tell all my LASIK patients they must wear eye protection when they play contact sports, and goggles when they swim. This is not my job. It is the job of the LASIK surgeon.
The bond between LASIK flap and cornea is so weak bacteria can easily creep under it and invade the cornea, even years after surgery. LASIK patients face a life-long risk their cornea flap will become infected.
A similar procedure, Photo Refractive Keratectomy, or PRK, also uses the excimer laser to reshape the cornea, but instead of a flap the surgeons scrape off the top layer of the cornea. PRK was the first procedure approved by the FDA to re-shape the cornea. Like LASIK, PRK is cosmetic.
PRK is more painful than LASIK, but PRK patients have one advantage over LASIK patients – they do not have a flap, so they do not get flap complications. Aside from this one advantage, PRK patients have the same complications as LASIK patients, plus they have a complication that LASIK patients do not have.
Most PRK surgeons treat the cornea with a chemotherapy agent called mitomycin-C (MMC) to decrease the risk of corneal haze after PRK. MMC kills corneal cells, so they do not grow back normally. This reduces haze, but at a price.
PRK patients are not informed an experimental chemotherapy agent known for causing mouth sores, hair loss and extensive tissue damage was applied to their eyes, with unknown long-term consequences. MMC has not been approved by the FDA for this use.
LASIK surgeons almost always pressure patients to have both eyes done on the same day. Some even offer discounts for the second eye. This violates a universally accepted rule of eye surgery – always let an operated eye heal for at least two weeks before you operate on the second eye.
Why do they do this? My guess is LASIK surgeons know when one-eyed LASIK patients compare the vision in their operated eye to their unoperated eye, they will immediately notice the operated eye has blurred vision, distortions, glare, etc., and it cannot discriminate between shades of grey. They will not schedule the second eye.
Ophthalmologists – including LASIK surgeons – measure visual acuity with high contrast black letters on a white background. This isn’t the way we see in the real world. Objects are not all pitch black with straight crisp sides against a white background. Our eyes need to distinguish between subtle gradations of color, brightness, and form in the real world.
LASIK surgeons define “success” as being able to see 20/40 using high contrast black letters on a white background without glasses. By this criterion, they claim the “success” rate of LASIK is 99%. They never ask the LASIK patients themselves. If they did, they would discover huge numbers of “successful” LASIK patients would not agree with their definition of “success”, even if they can see 20/40 in the LASIK surgeons”™ offices.
As of this writing, roughly 11 million people in the US have had LASIK. The exact number of complications is not known, because the LASIK surgeons refuse to report them.
The LASIK surgeons like to say with new improved techniques the complication rate has gone way down. Nonsense. The new techniques – like the old technique – invariably cut corneal nerves, thin the cornea, and cause scarring. Also, if LASIK surgeons refuse to report complications, how do they know the complication rate has gone down?
The evidence for the dangers of LASIK is hiding in plain sight. The Patient-Reported Outcomes with LASIK (PROWL) study, published in JAMA Ophthalmology in 2017, evaluated two groups of people before, and six months after, LASIK. Patients filled out a web-based survey about their vision before LASIK, and several times afterward.
The study showed that, overall, the ability to see small letters on the eye chart without glasses did improve after LASIK. However, the study also showed that forty-five percent of subjects who had reported no visual symptoms prior to surgery reported new symptoms three months after their surgery, including double images, glare, halos, and starbursts.
There was a flaw in the PROWL study: one of the pre-op questions was: “Do you have glare and starbursts WITH OR WITHOUT your glasses?” Almost all nearsighted patients – especially if they have astigmatism – will have glare, double vision, and starbursts WITHOUT their glasses. These symptoms disappear when they put their glasses on.
As expected, two thirds of the patients reported visual symptoms before the surgery, so these patients were excluded from those who developed “new symptoms” after surgery. Result: the study statistics are artificially lower than they should be. The researchers seem to have had a bias in favor of making LASIK appear safer than it is.
LASIK ads claim patients will be able to throw away their glasses after LASIK, and they will have perfect vision. Neither of these claims is true.
A 2009 Consumer Reports survey of seven hundred and ninety-three LASIK patients showed only one third of LASIK patients were able to stop wearing glasses. Two thirds continued to use glasses, or contact lenses, either some or all the time, either for distance, or reading, or both. The FDA website on LASIK correctly states: “Only a certain percent of patients will achieve 20/20 vision without glasses or contacts.”
The FDA website also states: “Some patients lose lines of vision that cannot be corrected with glasses or contact lenses.” The fact is ALL patients have distorted vision after LASIK, especially in dim light. Even LASIK patients who can see 20/20 without glasses do not have “perfect” vision.
Corneas have a single smooth curve before LASIK. During LASIK, the excimer laser flattens the center of this curve, so the cornea now has two curves – an artificially flattened curve in the center, and the original curve in the periphery.
In bright light, the pupil constricts, so LASIK patients look exclusively through the center of their cornea. Since this section has only one curve, their vision is less distorted than it is in dim light.
In dim light the pupil dilates, so two different curves come into play – the peripheral curve, and the central curve. The re-shaped central portion of the cornea focuses light directly on the retina. The untouched peripheral cornea focuses light either in front of the retina, or behind the retina. All LASIK patients inevitably see double or triple in dim light, with glare, starbursts, and halos.
LASIK patients are a danger to themselves and others in dim light. A case in point is airplane pilots.
Federal Aviation Administration regulations require a pilot’s distance vision to be 20/20 or better, with or without correction, in each eye separately. Nearsighted, farsighted, and astigmatic pilots must wear glasses or contact lenses when they fly.
The FAA allows patients who have had LASIK to fly planes if they have had a “successful outcome”, as measured by high contrast letters. The irony is the actual vision of LASIK pilots is not even close to normal – especially in dim light. All LASIK patients take a risk when they fly a plane, or drive a car, bus, or train at night.
All LASIK patients should have licenses that restrict them to driving or flying only during the day. I would not want to fly in a plane, or drive in a bus or a train, with a driver or pilot who has had LASIK in dim light. Nobody would.
Many patients I know had jobs where they had to work in dim light. After LASIK they became permanently disabled. One had to quit her job as a theatre critic because she could no longer see the actors when the lights went down. Another – an anesthesiologist – could no longer read charts in dim operating rooms. Another – a banker – can no longer work on a computer. She is on permanent disability.
The most feared LASIK complication is corneal ectasia, which is a relentless outward bulging of the cornea, rather like a hernia. Patients with thin corneas are at especially high risk of ectasia following LASIK. (In rare instances, ectasia is caused by a hereditary eye disease, keratoconus.) Again, most consent forms don’t mention, or explain, this devastating complication.
Ectasia is nasty. As the bulging becomes worse and worse, the eye becomes more and more nearsighted, and develops marked irregular astigmatism.
A LASIK surgeon said at a corneal meeting he never reported ectasia, because he was afraid of lawsuit. By February 2015, only 100 cases of ectasia had been reported in the world literature.
The world finally got a true picture of the risk of LASIK- induced ectasia in the US in 2016, when a company called Avedro went public. Avedro developed a procedure to stiffen the cornea by cross-linking collagen, which, they claimed, would halt the progression of ectasia.
Avedro’s procedure involves applying Riboflavin to the cornea, and then irradiating it for 30 minutes with ultraviolet light. This treatment does not work well, and it can seriously damage the cornea.
Avedro’s press release stated, “at least 160,000 patients in the U.S. have developed corneal ectasia following refractive surgery”. If you do the numbers, this means almost 1.5 percent of LASIK patients develop ectasia. Where did Avedro get the 160,000 number? It must have come from the LASIK surgeons themselves. They knew ectasia was a big problem, but they did not report it.
Now let’s talk about eye pain. I knew LASIK would cause pain, but I had no idea how bad it would be. The LASIK surgeons call this pain “dry eye”, although eyes with post-LASIK pain do not show any signs of dryness, such as corneal staining and tear debris. Instead, they look completely normal and well healed.
What these eyes really have is far worse than dry eye. They have corneal neuropathic pain. Neuropathic pain typically comes on well after the surgery – at least three months, and sometimes years, later.
Neuropathic pain is caused by damage to small nerves that run through the cornea. Their role is to keep it healthy. These nerves inevitably get cut during LASIK. They never grow back normally, and they develop persistent low-grade inflammation. In certain patients, the nerves start to fire constantly. This causes unrelenting, unbearable, untreatable pain. The same phenomenon can occur after a patient loses a limb. In this case it is called: “phantom pain.”
Neuropathic corneal pain causes severe foreign body sensation, burning, and dryness. Some LASIK patients put wetting drops in their eyes several times an hour, trying to alleviate the pain. Yes, I mean every hour. Walk into any drug store and you will see shelves of artificial tears labelled “For LASIK dryness.”
The irony is that these artificial tear drops do not help, because the eye is not dry. Post-LASIK corneal neuropathic pain is a type of Chronic Pain Syndrome, which you will read about in Chapter 26, “The Doctor Becomes a Patient”.
A bad LASIK outcome cannot be corrected. There is no way to get rid of glare and halos around lights at night. There is no way to restore contrast sensitivity. There is no way to eliminate post-LASIK pain. And there is no way to eliminate flap complications.
One LASIK surgeon I know said he no longer performs the procedure because – and I quote – “If something goes wrong, you can’t do anything about it”.
Dr. Ray Jui-Fang Tsai, an ophthalmologist who introduced LASIK to Taiwan, announced in 2012 he no longer performs LASIK. He has seen many patients who initially had a good result suffer rapid vision loss a decade later due to corneal flap inflammation, and/or corneal flap dislocation caused by poor healing.
The US scientific journals have joined in the conspiracy to hide LASIK complications from the public. They refuse to accept any papers that criticize LASIK. Almost all the papers about LASIK complications have been published in the international literature, not in the US literature.
Post-LASIK corneal neuropathic has been treated successfully in Europe with drugs like Amitriptyline. LASIK surgeons in the US refuse to perform any studies on how to treat this pain, because they refuse to admit this pain exists. Papers on this subject that are submitted to US journals are routinely rejected. Perry Rosenthal, a respected researcher at the Massachusetts Eye and Ear Infirmary in Boston, wrote many papers on chronic LASIK pain. They were all rejected.
Only a handful of US ophthalmologists treat LASIK corneal neuropathic pain. They include Pedram Hamrah at Tufts in Boston, Anat Galor at Bascom Palmer Eye Institute in Miami, and John Cason at the Naval Medical Center in San Diego.
There are thousands of MedWatch complaints about LASIK injuries on file with the FDA. Three quarters of them involve dry eyes (i.e., neuropathic pain), poor vision at night, and decreased visual acuity. There are over 1,200 signatures on a petition to stop LASIK. (See http://www.thepetitionsite.com.). Despite this evidence, the FDA refuses to revoke its approval of LASIK. This is the government agency whose primary responsibility is to protect the public.
LASIK represents the worst of American medicine. LASIK is not a healing profession; it is a business. Informed consent has been replaced by deceptive advertising. Disastrous outcomes are hidden from the public, and the system is rigged so that it is almost impossible to win a LASIK malpractice suit. The focus is not on helping the patient, but on helping the bottom line of LASIK surgeons.
The increasing number of malpractice suits against LASIK surgeons is giving ophthalmology a bad name. I am ashamed by my profession.
Bottom line: the less eye surgery, the better. All eye surgery has risks. No eye surgery should be done unless there is a pressing need. If an operation is necessary to save sight – retinal detachment surgery, for example – we accept the risk. Getting rid of glasses is not a pressing need.

